


Executive Summary
Mental health literacy (MHL) means understanding mental health issues and knowing how to recognize, manage, or prevent them. In the tech industry, high stress from deadlines, long hours, imposter syndrome, cognitive overload, and remote work can affect developers’ well-being (Wong et al., 2023). This article explains MHL’s components, why it matters for developers, common warning signs in the workplace, and evidence-based strategies to improve literacy. We cover practical steps teams can take – such as training, peer support, and workload management – and how to measure progress with surveys and feedback. We also note barriers (like stigma) and how leaders can overcome them. Two fictional case studies illustrate typical developer scenarios and positive outcomes. These approaches align with principles of Seligman’s PERMA model of well-being (Positive emotion, Engagement, Relationships, Meaning, Accomplishment), by promoting supportive relationships and meaningful work.
What Is Mental Health Literacy?
“Mental health literacy” refers to the knowledge and beliefs about mental disorders that help with their recognition, management, or prevention. In practice, it means knowing the common signs of stress, anxiety, depression, etc., understanding risk factors, knowing about self-help and professional treatments, and having positive attitudes toward seeking help. Key components include the ability to recognize symptoms or distress, knowledge of causes and treatments, knowing how to find information, and supportive attitudes that reduce stigma. Jorm (2000) defined MHL in this way and noted that many people cannot recognize disorders or know how to get help, and that stigmatizing attitudes often block people from seeking assistance. Thus, building Mental Health Literacy means educating employees so they and their peers can notice problems early and feel comfortable talking about them.
Developer-Specific Stressors and Mental Health
Software developers face unique pressures that make mental health literacy important. Tight deadlines and heavy workloads are common in tech, and studies show nearly 40% of workers report burnout driven by excessive tasks and poor support. For developers, constantly changing technologies and the need to keep learning can add to cognitive load. Research notes that when working memory is overloaded (for example, by too many tasks or interruptions), error rates rise and burnout symptoms appear. Similarly, imposter syndrome – feeling like a fraud despite evidence of competence – is widespread in tech and correlates with anxiety and depression. Takaoka et al. (2024) found that higher imposter feelings were linked to worse mental health among software engineers, and conversely, higher mental health literacy was linked to lower anxiety and imposter scores.
Remote work and isolation are further factors. While working from home can reduce commute stress, it can blur work-life boundaries and create loneliness. One survey found that developers reported higher rates of anxiety and depression than the general population. In another study, software engineers showed elevated burnout and even suicide rates compared to other information workers. All these stressors – long hours, on-call duty, imposter feelings, constant change, plus pandemic-related strains – mean developers need strong knowledge and support to stay well.
Recognizing Signs and Early Intervention
Early recognition of mental distress in the workplace is crucial. Common warning signs include sustained changes in performance or behavior. For example, an employee might miss deadlines or make more mistakes, struggle to concentrate, or suddenly work extreme overtime. They may call in sick more often or seem unusually late or fatigued. Emotional changes – frequent irritability, withdrawal from colleagues, tearfulness or mood swings – are also red flags. Leaders might notice physical complaints like headaches or poor self-care (e.g. weight change, unkempt appearance). Importantly, these should be seen as patterns over weeks, not single incidents. If an employee’s usual behavior changes dramatically, it may signal stress or depression.
Managers and peers should be trained to respond supportively. Best practice is a private, compassionate conversation: express concern (“I’ve noticed you’ve seemed stressed”) and listen, rather than dismissing or diagnosing. Avoid minimizing (“just push through it”) and focus on resources. For instance, mention the company’s Employee Assistance Program, or simply remind them it’s OK to seek help. In crises (talk of self-harm, for example), leaders should act immediately (call emergency services or connect to crisis lines) rather than ignore warning signs. Compassionate leadership and psychological safety – a climate where speaking up is encouraged – help people come forward with issues.
Strategies to Improve Mental Health Literacy
Research shows several evidence-based strategies can boost mental health literacy and well-being at work:
- Education and Training: Offering structured training sessions or workshops raises awareness. This can include general mental health literacy courses that teach how to spot symptoms, or mental health first aid training that equips people to help colleagues. In studies, such training improves knowledge and reduces stigma (Jorm, 2000). Training can be delivered online (self-paced courses) or in-person (HR sessions). Key content should cover common developer stressors (burnout, imposter syndrome, depression, anxiety) and practical self-help tips (sleep, exercise, break scheduling).
- Peer Support: Establishing peer networks can normalize talking about mental health. This might involve setting up regular informal check-ins or “buddy” systems, where team members support each other. Peer-led support groups have been effective in other workplaces for improving well-being and trust. When colleagues share coping strategies and encourage each other to take breaks or seek help, literacy naturally grows. For example, pairing junior developers with senior mentors can reduce imposter feelings and isolation, reinforcing PERMA’s Relationships and Engagement.
- Manager and Leader Training: Because managers play a key role, specific training for them is critical. Studies show that training managers in mental health leads to better team outcomes. When supervisors learn to recognize stress, talk openly about mental health, and approve reasonable accommodations (like flexible hours or reduced workload during crunch times), employees feel safer asking for help. One large UK study found that firms with more line manager mental health training saw higher staff retention and business performance, and lower long-term sickness absence due to mental health issues. This underscores that manager engagement in MHL is effective and has business benefits.
- Digital Tools and Resources: Providing easy-to-access digital tools can enhance literacy. These include mental wellness apps (meditation, CBT exercises), online counseling platforms, or curated resource libraries. Evidence suggests that self-guided digital interventions (e.g. stress-management programs, resilience training apps) can prevent burnout and improve well-being when chosen carefully. Employers might offer subscriptions to mental health apps or host virtual “wellness hubs.” Importantly, integrate these tools into the work culture – for instance, set expectations that staff can take short “mental health breaks” to use a mindfulness app or go for a walk.
- Reasonable Workload and Policies: Aligning policies with mental health goals is essential. Organizations should strive for manageable workloads (monitoring overtime, avoiding chronic crunch). High workload is a top burnout driver, so employers should ensure project timelines are realistic. Policies might include hard cut-off times to prevent all-night coding, or rotating on-call to share stress. Work arrangements (like remote days or flexible schedules) can accommodate personal needs (e.g. therapy appointments). Regular check-ins about workload and adjustments (job crafting) are shown to improve well-being. Such measures support PERMA’s Engagement (by keeping work challenging but not overwhelming) and Accomplishment (by enabling achievable goals).
- Psychological Safety and Culture: A culture of openness is foundational. Psychological safety – the belief that one can speak up without fear – reduces burnout and improves retention. Leaders can model this by openly discussing their own self-care (e.g. taking a mental health day) and not penalizing people for admitting struggles. Including mental health topics in regular meetings or internal newsletters can normalize them. Celebrating small wins and acknowledging effort can boost positive emotions (PERMA’s Positive Emotion). Surveys often find that stigma and fear of career harm are top barriers to seeking help, so explicitly combating stigma in communications helps build literacy. (Jorm 2000 noted that negative attitudes often block help-seeking.) Creating a “no-blame” environment when deadlines slip due to stress is also crucial.
Combining these strategies creates a more mentally literate and supportive workplace.
Figure 1 outlines key steps a development team can take to implement a mental health literacy program.
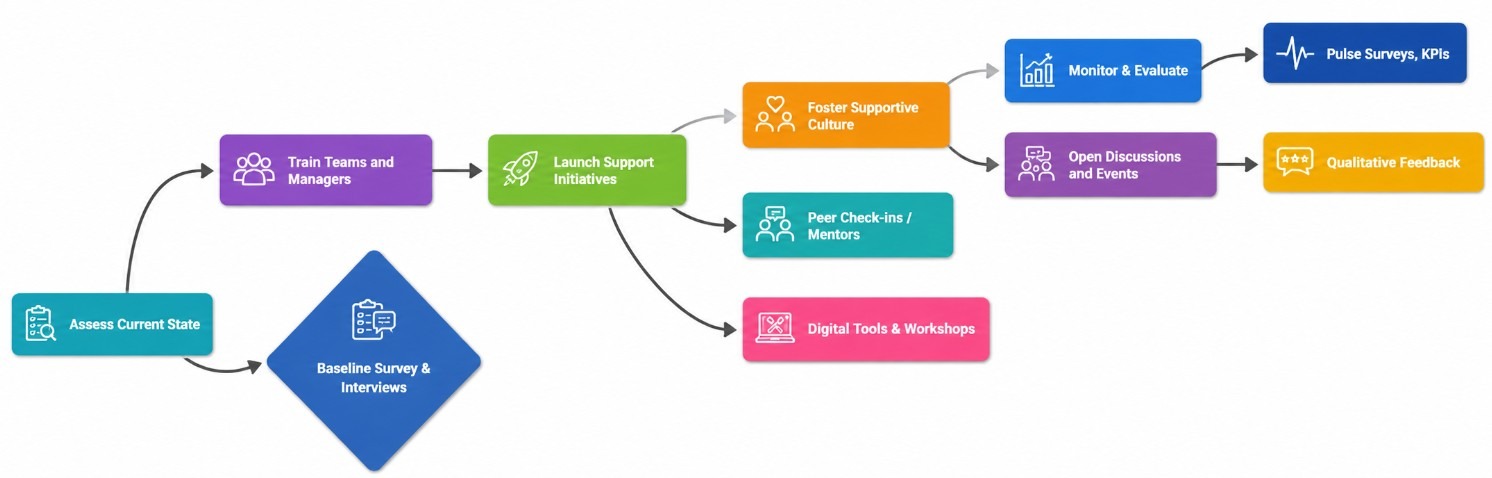
Figure 1: Steps for implementing a developer mental health literacy program
Practical Steps for Teams
In practice, software teams can take specific actions:
- Assess Needs: Survey your team anonymously about stressors and knowledge gaps. Include questions on workload, imposter feelings, and comfort with seeking help. This establishes a baseline for planning.
- Provide Education: Hold workshops or share online modules covering mental health basics, stress management, and company resources. Tailor examples to developers (e.g. “stressful sprints”). Encourage questions.
- Encourage Peer Support: Set up regular “virtual coffee” meetings or mental health check-ins where developers can share challenges informally. Consider a mentor system so that less experienced devs can discuss worries with a peer.
- Train Managers: Ensure team leads know how to respond to mental health issues. This might mean formal training, or at least guiding managers to listen empathetically, recognize signs, and know when to recommend resources.
- Promote Tools: Distribute information about apps or EAP services. For example, send a periodic “wellness tip” email or Slack message with links to meditation apps or counseling hotlines.
- Manage Workload: Actively track project timelines. If someone regularly works late or shows signs of strain, redistribute tasks or adjust deadlines. Encourage regular breaks (e.g. Pomodoro technique) and use of paid time off.
- Build Psychological Safety: Model vulnerability. For instance, lead by example and take occasional mental health days or share that “it’s OK not to be OK.” Celebrate when team members use wellness resources.
- Monitor Outcomes: Periodically measure progress. After interventions, conduct follow-up surveys on stress, burnout, and satisfaction. Track metrics like sick-day rates or turnover. Solicit qualitative feedback on what’s working.
By iterating these steps and keeping literacy high, teams help prevent crises and improve well-being and productivity together.
Measuring and Evaluating Efforts
To know if mental health literacy improves, use both quantitative and qualitative measures. Employee surveys are key: brief pulse surveys can track changes in stress levels, burnout symptoms, or confidence in accessing support. For instance, ask how comfortable people feel discussing mental health at work, before and after training. Compare metrics over time – for example, aim for fewer sick days or fewer people working excessive overtime. KPIs might include rates of EAP usage or completion of mental health training courses. Qualitative feedback (focus groups or interviews) provides context: developers can suggest what resources helped. It’s also useful to monitor project outcomes – teams with a healthy culture often see more consistent delivery and fewer bugs related to fatigue. In all cases, ensure anonymity and confidentiality so employees give honest feedback.
Barriers and Overcoming Them
Implementing MHL faces challenges. Stigma and Fear are perhaps the biggest: even if resources exist, developers may worry that admitting stress will mark them as weak or hurt their career. To counter this, senior leadership must endorse mental health openly and protect confidentiality. Making training mandatory or highly visible shows organizational commitment. Time Constraints can be a barrier – teams might feel they “can’t afford” time off or training. To overcome this, integrate mental health time into work (e.g. scheduled wellness breaks) and highlight long-term gains (trained managers, reduced burnout means less churn and higher quality). Resource Limits (budget or personnel) can limit fancy programs, but many strategies are low-cost: peer support groups, open discussions, or trial of free apps. Even short lunch-and-learn sessions count.
If projects are urgent, teams can use the RADAR approach (Review, Adjust, Discuss, Act, Reassess) to slot in quick check-ins. Finally, some developers may mistrust wellness programs as “HR propaganda.” Honest co-creation can help: involve team members in planning mental health initiatives so they address real needs. Emphasize that mental health is part of overall performance and safety, just like ergonomics for physical health. By normalizing these efforts, barriers can be reduced.
Alignment with PERMA Model
Many of these practices align with the PERMA model of well-being (Seligman, 2012). For example, building Positive Relationships (R) through peer support groups and team check-ins helps developers feel connected and cared for. Encouraging Engagement (E) can mean ensuring developers work on meaningful tasks at an appropriate pace, avoiding endless context-switching. Providing Meaning (M) might involve reminding teams how their work impacts users or society, countering cynicism. Facilitating experiences of Accomplishment (A) – by celebrating completed projects and setting realistic goals – boosts confidence and reduces imposter feelings. Finally, promoting Positive Emotions (P) is achieved when managers show empathy and create an uplifting environment (e.g., sharing small successes, supporting a work-life balance). Together, Mental Health Literacy initiatives support the full PERMA framework, leading to both better mental health and more resilient, flourishing teams.
Fictional Case Studies
The following fictional case studies illustrate how developer teams might apply mental health literacy in practice, and the positive outcomes that can result.
- Case 1 – Remote Developer with Imposter Syndrome: Alex is a mid-level software engineer working fully remotely. Over months, Alex feels “not good enough” compared to colleagues, works evenings to catch up, and starts missing deadlines due to burnout. His anxiety grows, but he is reluctant to tell his manager (fear of judgment). Intervention: The company offers a virtual mental health literacy workshop (covering imposter syndrome and stress management) and sets up small peer support groups on Slack. Alex’s manager also attends manager training and learns to check in with team members. Colleagues share their own struggles in a team meeting, normalizing the issue. Outcome: Alex realizes others feel similarly, shares his workload concerns, and takes advantage of flexible hours and a meditation app offered by HR. Within weeks, his self-confidence improves, he meets project deadlines again, and reports less anxiety. (PERMA elements: R, P, A)
- Case 2 – Onsite Developer Facing Burnout: Priya is a senior developer in a busy startup. Recent product deadlines have led to 60-hour workweeks. She is constantly tired, has trouble sleeping, and snaps at teammates. Her coworkers notice she’s withdrawn. Intervention: The dev team’s leaders institute a mental health check-in routine during daily stand-ups. Priya’s manager attends mental health training and recognizes burnout signs. The team reassigns some of Priya’s tasks and enforces a policy of no emails after 6 pm. The company introduces a weekly group mindfulness session. Outcome: Priya starts leaving work on time, begins attending the mindfulness sessions, and even takes a mental health day off. Over the next month, her mood improves, her productivity stabilizes, and she feels more engaged. The overall team stress drops, and fewer bugs are reported. (PERMA elements: E, R, P)
Table 1: Comparison of the two fictional case studies, their interventions, and outcomes.
| Scenario | Intervention | Outcome |
| Remote dev with imposter syndrome and burnout signs | Virtual MHL workshop; peer support groups; manager check-ins; flexible hours and meditation app | Improved confidence, deadlines met, reduced anxiety; feels supported (PERMA: R, P, A) |
| Onsite dev facing heavy workload and stress/burnout | Manager mental-health training; reduced tasks; no-email policy; mindfulness sessions | Better sleep, higher engagement, sustained productivity, stronger team morale (PERMA: E, R, P) |
Conclusion
Mental health literacy is crucial in tech workplaces. By understanding what MHL entails and recognizing the specific stressors developers face (deadlines, imposter syndrome, cognitive load, etc.), teams can put in place effective supports. Evidence-based strategies – education, peer support, leader training, digital tools, workload management, and a culture of safety – can significantly improve early detection of issues and overall well-being. Practical steps such as regular surveys, check-ins, and training programs make MHL actionable. Measurement through surveys and KPIs keeps efforts on track. While barriers like stigma are real, they can be overcome with leadership commitment and open communication. Importantly, these efforts not only prevent problems but also foster positive emotions, engagement, meaning, relationships, and accomplishment (PERMA) in the workplace. In sum, integrating mental health literacy into a development team’s culture leads to healthier, more productive, and more resilient developers and organizations.
References
- American Psychiatric Association. (2023). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
- Burns, J. R., & Rapee, R. M. (2006). Adolescent mental health literacy: Young people’s knowledge of depression and help seeking. Journal of Adolescence, 29(2), 225–239. https://doi.org/10.1016/j.adolescence.2005.05.004
- Jorm, A. F. (2000). Mental health literacy: Public knowledge and beliefs about mental disorders. British Journal of Psychiatry, 177(5), 396–401. https://doi.org/10.1192/bjp.177.5.396
- Jorm, A. F. (2012). Mental health literacy: Empowering the community to take action for better mental health. American Psychologist, 67(3), 231–243. https://doi.org/10.1037/a0025957
- Keyes, C. L. M. (2002). The mental health continuum: From languishing to flourishing in life. Journal of Health and Social Behavior, 43(2), 207–222. https://doi.org/10.2307/3090197
- Maslach, C., & Leiter, M. P. (2016). Understanding the burnout experience: Recent research and its implications for psychiatry. World Psychiatry, 15(2), 103–111. https://doi.org/10.1002/wps.20311
- Organisation for Economic Co-operation and Development. (2021). Fitter minds, fitter jobs: From awareness to change in integrated mental health, skills and work policies. OECD Publishing. https://doi.org/10.1787/a0815d0f-en
- Seligman, M. E. P. (2011). Flourish: A visionary new understanding of happiness and well-being. Free Press.
- Shanafelt, T. D., & Noseworthy, J. H. (2017). Executive leadership and physician well-being: Nine organizational strategies to promote engagement and reduce burnout. Mayo Clinic Proceedings, 92(1), 129–146. https://doi.org/10.1016/j.mayocp.2016.10.004
- World Health Organization. (2022). World mental health report: Transforming mental health for all. World Health Organization. https://www.who.int/publications/i/item/9789240049338
- Yıldırım, M., Arslan, G., & Wong, P. T. P. (2022). Meaningful living, resilience, affective balance, and psychological health problems among Turkish young adults during coronavirus pandemic. Current Psychology, 41, 7812–7823. https://doi.org/10.1007/s12144-020-01244-8