


Introduction
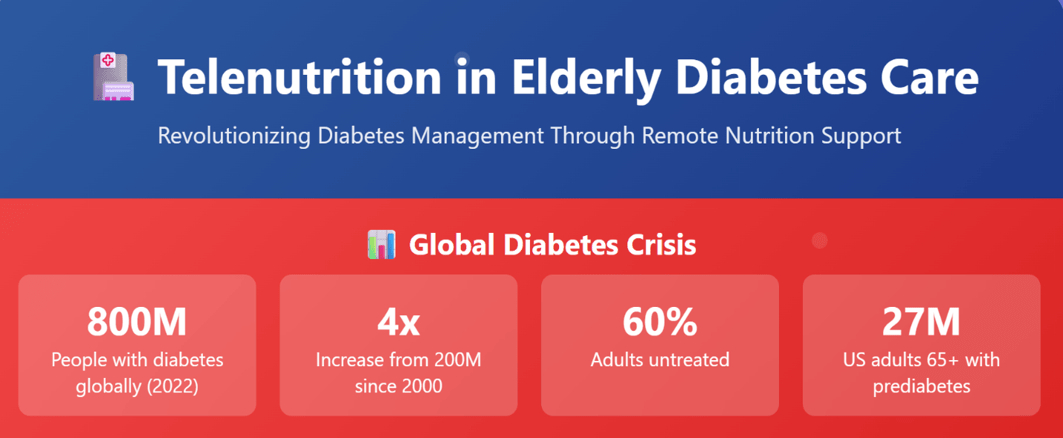
According to the WHO, the number of people suffering from Diabetes has quadrupled, going from 200 million people to 800 million in 2022. At the same time, 450 million were adults, and approximately 60 percent were untreated. One of the most affected is Southeast Asia and Eastern Mediterranean, as well as Africa, which has the lowest treatment rate, meaning that less than 4 patients out of 10 are under medication (Global Diabetes Epidemic Reaches Critical Levels With 800 Million Cases, 2024).
According to Diabetes research, almost 27 million people aged 65 years or older suffer from prediabetes in the US, and the incidence of diabetes diagnosis was higher in the age population between 45 and 64 years and patients over 65 years old compared to younger adults. Moreover, Diabetes was found to be the number one cause of blindness in the age population around 18 to 64 years old, additionally associated with a medical cost per person of $8000 to $9000 American dollars. (Diabetes Research Institute Foundation, 2023).
The Nutritional Vulnerabilities of Older Adults with Diabetes
As the global population ages, elderly patients with Diabetes are prone to develop complex clinical complications, including hypertension, blindness, and kidney disease. To maintain glycemic control for older adults is more than medications; it largely relies upon nutrition. But growing older causes changes physiologically, cognitively, and psychosocially, so managing nutrition represents a challenge.
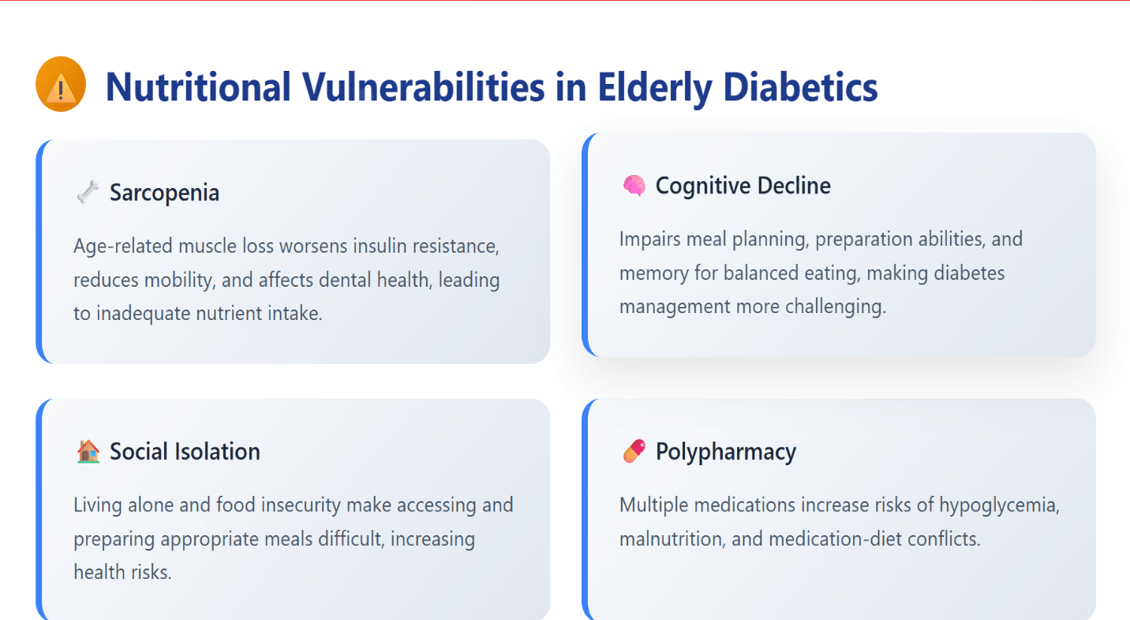
Sarcopenia, as muscle mass is lost due to age, can worsen insulin resistance and reduce mobility, affecting dental health. It can also cause changes in appetite and often lead to inadequate nutrient intake. Cognitive decline and early dementia may impair the ability for planning and preparing. Eating balanced meals may also become difficult to remember. Additionally, many elderly patients live alone or face food insecurity, and this situation makes it harder to access or prepare appropriate meals. These vulnerabilities add to the risk for hypoglycemia, malnutrition, and medication-diet conflicts. These risks can worsen through polypharmacy.
Proactive, individualized nutrition interventions are important, so they are required for clinicians. A solution that is timely and also effective is Telenutrition for providing nutritional monitoring and counselling through remote technologies.
Recent advancements with telehealth have transformed the landscape of diabetes management because they offer alternative approaches to customary in-person care. Telehealth interventions include telenutrition also videoconferencing that aim to improve upon glycemic control, promote healthier behaviors as well as increase healthcare accessibility, notably in remote or underserved areas. In Nutrients, there was a 2024 study that was published. It shows telenutrition based in videoconferencing can effectively provide education that is an alternative to in-person education for those with type 2 diabetes mellitus (T2DM). Additionally, telehealth approaches improve diets through reducing energy, carbohydrate, and salt intake, which further manage glycemic levels (Mori et al., 2024).
Telenutrition as a Clinical tool: Evidence and Use Cases
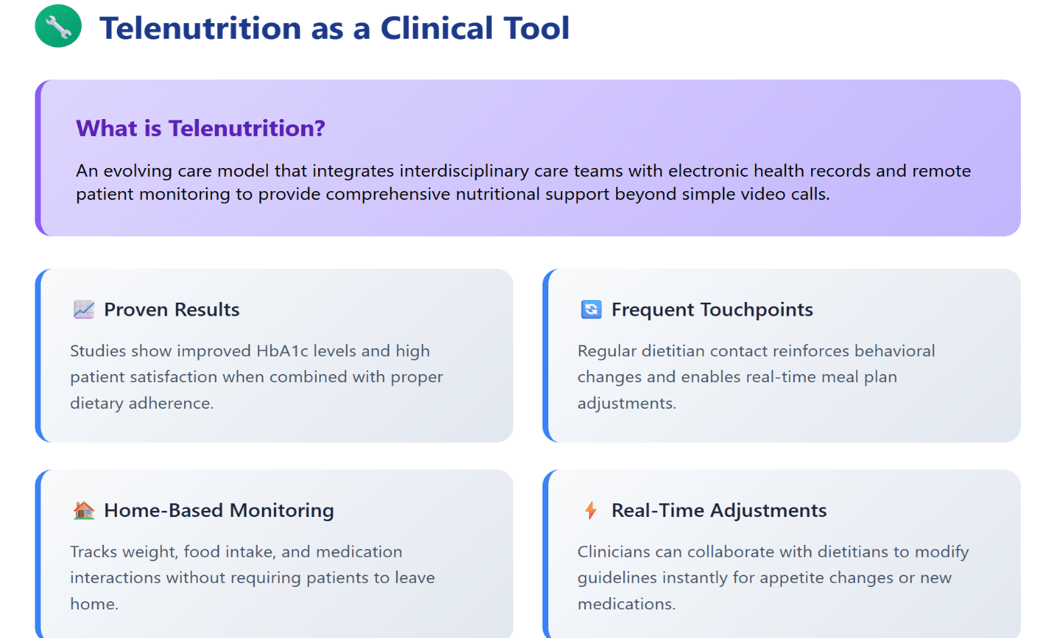
Telenutrition involves so much more now than just calling dietitians via video. Within this evolving care model the interdisciplinary care teams integrate themselves into electronic health records and remote patient monitoring. Evidence can support its use for the management of type 2 diabetes because of how various studies show that HbA1c levels do improve when diets are followed well, plus patients are satisfied (Mori et al., 2024).
Telenutrition provides for more frequent touchpoints between dietitians alongside elderly patients therefore this helps to reinforce small behavioural changes plus to adjust meal plans without delay. Weight, food intake, and medication-nutrient interactions require active monitoring that enables it. Because of this, the patient does not have to leave their home. For example, a clinician could work together with a dietitian in order to adjust diet guidelines in the event loss of appetite occurs or a patient uses a GLP-1 agonist.
Telehealth is helpful and specifically Telenutrion in Elderly Diabetes Care. It has but one merit being lab unaware data. It aids patients via support that is ready and furthermore keen. Then such motivation can sustain the changed behaviors. Telehealth offers logistical benefits such as reduced travel time and lower costs, and patients find more convenience, so that regular follow-up becomes feasible. Throughout the COVID-19 pandemic period, telehealth was indeed valuable since it ensured care went on while infection risks got minimized. Furthermore, videoconferencing allows for visual and auditory communication as well, and this can make people adhere to it as well as understand it more than voice-only interventions.
Empowering and engaging the Patients and family members
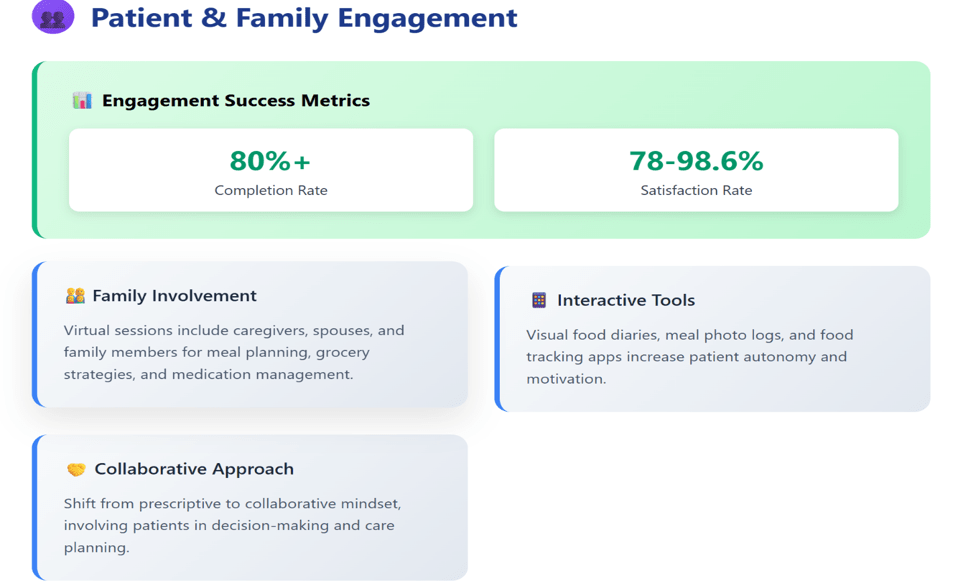
High levels of patient adherence and engagement, researchers report, appear in telenutrition studies showing over 80% completion. Participants were satisfied because convenience along with ease of use in addition to motivation besides accountability plus personalized support eased them, ranging from 78% to 98.6%. Certain dropout cases were attributable to the challenges some participants experienced like lack of personal contact as well as difficulties with technology use plus self-monitoring despite these positive indicators. These perceptions underscore the reasons why platforms should be user-friendly for people. Furthermore, tailored dialogue matters to sustain involvement (Daud et al., 2025).
Elderly patients rarely manage diabetes by themselves. For meal preparation and grocery shopping along with medication management caregivers such as spouses, adult children, or professional aides often see active roles. Telenutrition is an opportunity for engagement with these stakeholders in care because it improves communication and adherence.
Clinicians recommend virtual nutrition sessions for family members or caregivers. They can create useful plans together during these sessions. This might include meal prepping during the week or understanding the impact of certain foods on blood sugar levels. One more item might be an overview of food tracking app usage. Caregiver burden can be reduced so confidence is improved with this approach.
Additionally, patient involvement occurs during decision-making, including online choices that foster self-determination and respect. Patients are able to play an active role in their care through using tools like visual food diaries or meal photo logs, so this active role has been shown to increase motivation plus outcomes. It means clinicians shifting toward a collaborative from prescriptive mindset.
Making It Simple: Tech Tips for Older Adults and Clinicians
One of the perceived barriers to Telenutrition in Elderly Diabetes Care is also that older adults use technology. However, many of these concerns are overstated. Digital health tools are able to allow seniors to engage effectively with the right support and with guidance.
Tech-readiness assessment is where clinicians should begin. Can the patient access use a smartphone, tablet, or computer? Is the internet with them reliable? Do they need minimal assistance for opening and using apps or video calls? Clinicians can make recommendations for platforms that are matching of the patient’s capabilities based on these answers.
Some tips include
- For recommending of simple navigation and apps with large fonts.
- Platforms not needing logins as well as downloads may be used. Texted or emailed secure links how good examples.
- Using voice-activated assistants (like Alexa or Google Home) is encouraging as reminders
- Aides at home can help caregivers. The devices should be set up prior to the appointments with them.
In order to strengthen tech adoption, digital health navigators or social workers may be requested by clinicians in certain cases. Continuous care of the patient is ensured, and drop-off is prevented by building in this support at the beginning.
Primary care micropractices that aim to improve patient engagement and continuity of care should begin through carefully selecting virtual care technologies which align with their workflow and patient needs. Necessary tools include virtual appointment platforms such as RingCentral, online booking systems like Veribook, and Electronic Medical Records (EMR) systems including Med Access EMR (Telus Health). A tethered patient portal such as Pomelo Health integrates, and it is also critical for enabling secure messaging when it schedules appointments, when it sends reminders, and when it shares information. The EMR contains these tools, so a hybrid care model is easily supported. Due to this centralization transitions between in-person plus virtual visits become smooth (Burton et al., 2022).
From Screens to Success: Building Consistency
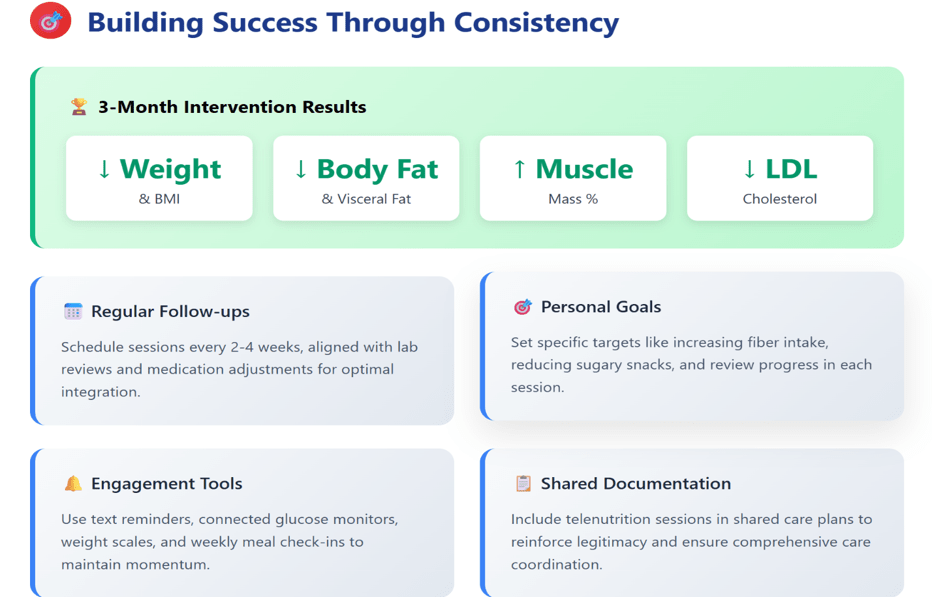
Recent studies have demonstrated that overweight together with obese adults greatly improve metabolic health markers and weight loss through nutritional counseling plus personalized health coaching when combined with telemonitoring. After around three months, participants that were receiving all of these integrated interventions showed more prominent reductions in terms of their weight, body mass index (BMI), body fat percentage, visceral fat, and of course their waist circumference (WC). The muscle mass percentage did also increase during this time. Additionally, biochemical markers such as blood triglycerides as well as low-density lipoprotein (LDL) cholesterol levels improved greatly in the intervention groups, plus this indicated improved cardiovascular risk profiles. These gains showed up mostly at three months, gains were still there at six months, though numbers mattered less over time.
Multidisciplinary teams with physicians, dietitians, and also health coaches do get involved so strongly. These interventions then become successful afterward. Health coaches play a pivotal role as they set specific goals and also provide motivation plus support dietary adherence through using telemonitoring data in personalized one-on-one online sessions. Participant engagement is improved via this collaborative approach ensuring continuous follow-up and tailored counseling optimizing outcomes beyond telemonitoring alone (Eid et al., 2024).
As with any behavioural intervention, the key to success is consistency. For telenutrition’s effectiveness, telenutrition must be a regular part of the patient’s routine, not a one-off.
Clinicians can have a role within normalizing this
Key Suggestions:
- Schedule regular follow-ups every 2 to 4 weeks.
- Clinicians align telenutrition visits for lab reviews or medication adjustments.
- We encourage patients as they set personal goals such as when they increase fiber intake, when they reduce sugary snacks, and as we review progress in each session.
Simple tools such as text reminders, RPM integration (e.g., weight scales or connected glucose monitors), or weekly meal check-ins can sustain engagement. Small wins like stable post-meal glucose readings or better energy levels keep patients motivated.
Clinicians should likewise share documentation from telenutrition sessions within the shared care plan because it reinforces legitimacy also ensures dietitians actively participate in the broader clinical picture.
In the end, Telenutrition in Elderly Diabetes Care also includes more aspects than just solely food. Overall wellness is what it considers. Continuity accessibility and trust are what it’s all about. It gives some access to some personalized support for those elderly patients with diabetes. This support meets them at their physical, emotional, and clinical location.
Key takeaways
Clinical purpose of Telenutrition
- Integrates into EMRs and interdisciplinary care teams
- Continuous support and real-time meal plan adjustments with frequent dietitian check-ins
Engaging Patients and Relatives
- Virtual visits should involve with caregivers regarding for grocery strategies and for app use. These virtual visits should cover meal planning too.
- Visual food diaries along with meal photo logs can encourage patient autonomy. Co-designed plans also can do so.
- Motivational interviewing plus respectful collaboration is how trust builds.
Tech Tips for Elder Patients
- Assess tech access and reliability
- Recommend user-friendly platforms
Build Routine
- Schedule continus session aligned with clinical goals
- Keep track of progress (calories intake, DASH diet, improved glucose levels)
- Stablish reminders and share meal plans and session notes.
References
- Burton, L., Rush, K. L., Smith, M. A., Davis, S., Echeverria, P. R., Hidalgo, L. S., & Görges, M. (2022). Empowering patients through virtual care delivery: qualitative study with micropractice clinic patients and health care providers. JMIR Formative Research, 6(4), e32528. https://doi.org/10.2196/32528
- Daud, N. L. H. M., Nor, N. M., Jaafar, N. H., Bakar, W. a. M. A., & Shukri, N. a. M. (2025, March 25). The Feasibility and Effectiveness of Telenutrition for Remote Dietary Consultation: A Systematic review and Meta-analysis. https://www.foodandnutritionjournal.org/volume13number1/the-feasibility-and-effectiveness-of-telenutrition-for-remote-dietary-consultation-a-systematic-review-and-meta-analysis/
- Diabetes Research Institute Foundation. (2023, October 10). Diabetes Statistics – DRIF. DRIF. https://diabetesresearch.org/diabetes-statistics/
- Eid, N. M. S., Al-Ofi, E. A., Enani, S., Mosli, R. H., Saqr, R. R., Qutah, K. M., & Eid, S. M. S. (2024). Effects of a Telenutrition Weight Loss Program Supported with Telemonitoring and Telehealth Coaching on Anthropometric and Biochemical Measures in Overweight and Obese Adults: A Pilot Randomized Controlled Trial. Healthcare, 12(23), 2362. https://doi.org/10.3390/healthcare12232362
- Global diabetes epidemic reaches critical levels with 800 million cases. (2024, November 14). UN News. https://news.un.org/en/story/2024/11/1156971
- Mori, H., Taniguchi, S., Tamaki, Y., Tamaki, M., Akehi, Y., Kuroda, A., & Matsuhisa, M. (2024). Telenutrition Education Is Effective for Glycemic Management in People with Type 2 Diabetes Mellitus: A Non-Inferiority Randomized Controlled Trial in Japan. Nutrients, 16(2), 268. https://doi.org/10.3390/nu16020268